3D Printing Cardiovascular Anatomy: A Single-Centre Experience
3D PRINTING IN MEDICINE AND CONGENITAL HEART DISEASE
3D printing technology represents an extraordinary innovation, which has been compared to a ‘second industrial revolution’ [1]. In May 2015, an article in the Harvard Business Review commented that ‘industrial 3-D printing is at a tipping point, about to go mainstream in a big way. Most executives and many engineers don’t realise it, but this technology has moved well beyond prototyping, rapid tooling, trinkets, and toys’ [2]. Indeed, applications of 3D printing technology now range from the automotive industry to archaeology, from eyewear and fashion design to medicine. It is the medical field that experts in the sector indicate as the area in which the technology will play a really substantial and potentially revolutionary role in the coming years [3]. But 3D printing has been used for medical purposes well before recent technological advances and the press hype that ensued, with highly sensational titles in the media along the lines of ‘3D printer saves baby’s life’ [4]. Examples of medically relevant 3D models date back to the 1990s. Areas of medicine in which 3D printing technology can play an important role include manufacturing maxillofacial implants [5], personalising orthopaedic prostheses [6], creating patient-specific implants for craniofacial surgery [7], and even reconstruction of wound models for forensic purposes [8]. From renal [9] to cardiovascular [10], a range of models has now been manufactured and described, based on the underpinning principle that 3D printing technologies allow to print patient-specific models reconstructed from volumetric medical imaging data, based on a processing framework discussed in more detail elsewhere [11] and summarised in Figure 1.
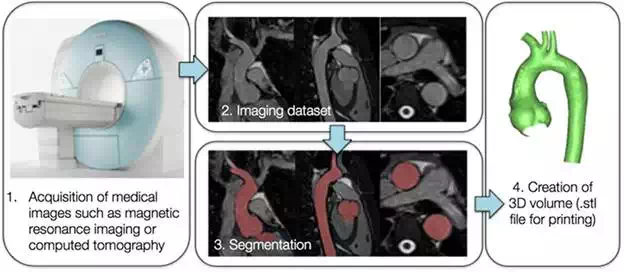
FIGURE 1.
Framework for 3D printing cardiovascular 3D models, starting from medical imaging acquisition (1), processing the image dataset with appropriate software (2 and 3) and generating a 3D volume (4) in a format compatible with the 3D printer.
The principle of being able to reconstruct patient-specific anatomical models and manufacture them by means of 3D printing (additive manufacturing, in particular) is especially appealing in the field of congenital heart disease (CHD). Patients with CHD are in fact born with complex, often unique, vascular and/or intra-cardiac anatomical arrangements. Parts of these complex anatomies get further manipulated and modified following cardiac surgery, with vessels being transposed, baffles being created, narrowed (i.e. stenosed) vessels being enlarged and whole areas (e.g. right ventricular outflow tract) being augmented by patches. The same patient can also receive implantation of cardiac devices, such as stents, valves prosthesis or occluder devices, during catheterisation procedures. Overall, the resulting unique scenario certainly warrants a patient-specific approach, which can be beneficial for different purposes:
● Appreciation of anatomy for patients selection or device selection
● Experimentation for better appreciation of the physiology and haemodynamics
● Opportunity to practice new procedures and test new devices
● Design of novel training and communication tools
Based on this rationale, the cardiac engineering team within the Centre for Cardiovascular Imaging at Great Ormond Street Hospital for Children (London, UK) has advocated a patient-specific approach for studying and potentially treating CHD for several years now. In this light, 3D printing technology has been used extensively and for different purposes, focusing on the potential translation of the technique in the clinical realm. This chapter briefly presents an overview of the Centre’s experience with 3D printing CHD, in order to create a showcase of the potential of the technique in the field. It will therefore touch upon clinical case studies, engineering experiments, and patients & public involvement and engagement (PPI/E).
Early experience: testing a novel cardiovascular device
One important application of 3D printing in CHD is represented by aiding in patient selection for specific procedures. In this context, the usefulness of 3D-printed models was assessed specifically for evaluating shapes and sizes of the right ventricular outflow tracts (RVOTs) in patients that would be possible candidates for percutaneous pulmonary valve implantation (PPVI). As a Centre leading in the introduction of PPVI in clinic [12] as well as its evaluation with engineering analyses [13], 3D printing patient-specific models represented an additional valuable tool for determining PPVI suitability. A study [14] demonstrated that having access to 3D models in addition to cardiovascular magnetic resonance (CMR) imaging data resulted in cardiologists improving the indication of patients suitable for implanting the first PPVI device (Melody® valve, Medtronic Inc) (Figure 2).
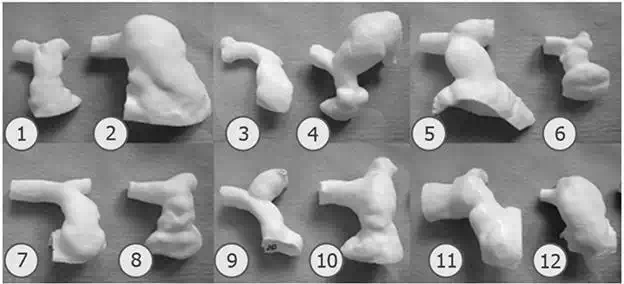
FIGURE 2.
Example of 3D-printed RVOTs from 12 patients [ref].
Within the context of PPVI and in relation to early observation on the first generation device being suitable for only a small portion of patients requiring pulmonary valve replacement, a novel device was developed. The latter was designed with the intention of fitting more dilated RVOTs. In this case, a patient-specific 3D model resulted extremely valuable for practicing device insertion prior to performing the first implantation of the novel device on compassionate grounds (i.e. first-in-man procedure). A candidate (42-year-old male) presented with a history of cardiac surgeries, deemed not suitable for additional surgery, and, however, still presenting with severe pulmonary regurgitation. The morphology and dimensions of his RVOT suggested that the second-generation PPVI device would have been suitable. A model was created from his computed tomography (CT) examination and 3D printing. As shown in Figure 3, the cardiologist was then able to use the model to practice device insertion and deployment prior to the procedure. Particularly, having access to the model allowed the cardiologist a) to guide device personalisation to assure safe anchoring in the specific anatomy and b) to identify a problem in deploying the device if accessing via the right pulmonary artery—conventional approach—while he could successfully deploy it when inserting the line via the left pulmonary artery. The latter strategy was used (successfully) on the day of the procedure [15].
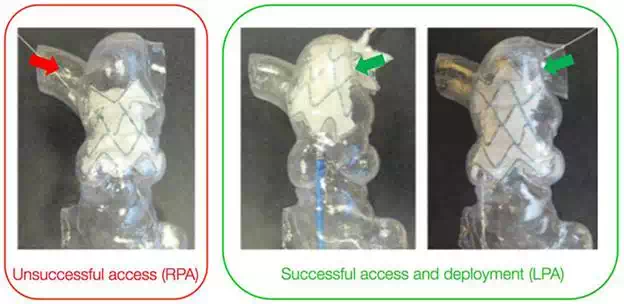
FIGURE 3.
A 3D-printed model was used for testing insertion and deployment of a novel device (second-generation, self-expandable PPVI stent). As a valuable practice tool, testing the procedure in the model is allowed to identify an unfeasible access route. LPA, left pulmonary artery; RPA, right pulmonary artery. . Stent diameter at extremities = 40.7 mm.
Models for decision support: a case study
By establishing a conversation with clinicians and embedding the technology within the hospital, it is possible that complicated cases requiring additional insight are brought to the attention of the engineer for the creation of a model, which could be either a computer simulation or a 3D-printed model, or both. The model is created specifically to appreciate features that have clinical implications. An interesting example is represented by a patient (19-year-old male) who presented a diagnosis of aortic coarctation, previously stented, and also had an aberrant left subclavian artery originating from the stent site. The discussion revolved around the possibility of inserting a Cheatham Platinum (CP) covered stent within the existing device to prevent formation of a small developing aortic aneurysm, without occluding the aberrant subclavian artery. Insight into the relative position of all these components was therefore desirable, and a model was reconstructed from CT data, including the stent. The aorta was printed in transparent rigid resin, while the stent was printed using a white stereolithography (SLA), therefore being easily identifiable within the anatomy. Furthermore, a cut was performed alongside the thoracic/descending aorta such that the model could be easily opened and, if necessary, to gather additional measurements. The model (Figure 4) contributed to assess the feasibility of the intervention highlighting the spatial relationship between stent, aneurysm and left subclavian artery. Additional computational analyses (including the same 3D domain) were performed to simulate the implantation of the CP-covered stent and the local fluid dynamics post implantation [16]. The intervention was performed successfully.
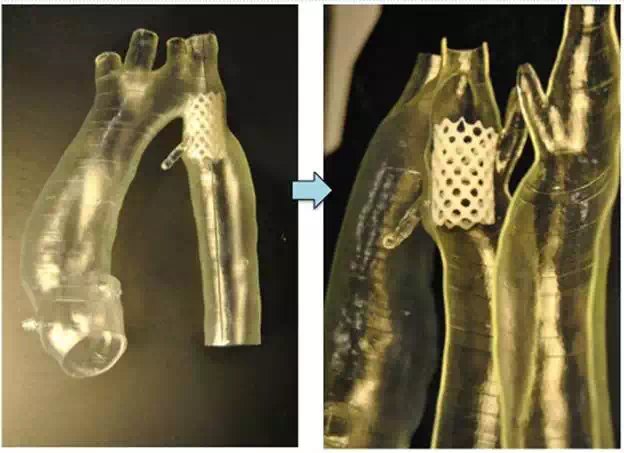
FIGURE 4.
Patient-specific 3D model of stented coarctation, printed with two different materials to better highlight the position of the device (length = 28 mm), including the possibility of opening the model to better appreciate the relative position of the stent with respect to the rest of the anatomy.
Developing patient-specific models for research purposes
The possibility of printing 3D patient-specific CHD models is appealing not only for important clinical applications (e.g. testing devices and procedures) but also for research purposes. Models can in fact be incorporated into experimental setups for the detailed analysis of local fluid dynamics and for overall hydrodynamic measurements. This is of particular relevance in CHD patients, as often in vivo measurements are not feasible or, if feasible, are technically challenging, e.g. measuring pressure-volume loops in single ventricle patients [17]. The use of appropriately tuned experimental systems has the advantage that parametric studies can be performed in a controlled and reproducible setting, i.e. changing one variable at a time incrementally. This can generate hydrodynamic data which can increase the understanding of complex physiology.
MULTI-SCALE HYDRODYNAMIC SETUPS: STUDYING SINGLE VENTRICLE PATIENTS
Patients with single-ventricle physiology (e.g. hypoplastic left heart syndrome, HLHS) present with a fragile physiology, as their cardiovascular system relies on a single pumping chamber supporting both the systemic and pulmonary circulations [ref ]. Hydrodynamic measurements are relevant to assess the effect of comorbities, e.g. aortic coarctation, on the fluid dynamics, as well as accurate measurements of quantities that are difficult to acquire in vivo, e.g. pressure drop in the surgically enlarged aorta in patients with palliated HLHS. To this end, a mock circulatory loop (MCL) can be constructed, whereby the cardiovascular system is experimentally summarised by appropriately tuned resistive and compliant elements. A system was built [18] using a Berlin Heart® ventricular assist device to simulate the single ventricle, and 3D-printed patient-specific models were manufactured and ‘plugged’ into the MCL to perform parametric experiments. This allowed us to test different aortic morphologies in the same controllable setup, e.g. tubular aortic arch, aortic arch with a severe coarctation, or an aortic arch in which the patching performed during the Norwood procedure had resulted in a very dilated transverse arch therefore creating a size mismatch with the descending aorta. 3D models are shown in Figure 5. Data on pressure drop along the aorta or flow distribution (upper body, lower body, pulmonary circulation) can be obtained using catheters and flow probes. MCLs can also be modified to simulate different surgical procedures. In the case of HLHS, for example, different surgical options exist to perform the first palliative procedure, i.e. different shunts can be used to source pulmonary blood flow to the pulmonary circulation. An MCL was built simulating first-stage palliation of HLHS with a modified Blalock-Taussig shunt [18] from the innominate artery to the pulmonary bed of the circuit and then modified to simulate first-stage palliation of HLHS with a Sano shunt [19] from the ventricle itself (in the experimental setup, from the de-airing valve of the Berlin Heart®) to the pulmonary bed of the circuit. The coupling of a detailed 3D model with a circuit summarising the remainder of the circulation can be considered a multi-scale [20] in vitro modelling approach for CHD. With regard to HLHS palliative surgery and the valuable insight that can be gathered experimentally, MCLs can be modified to incorporate the effect of respiration [21] which becomes relevant when these patients receive their second and third surgeries, i.e. the Glenn procedure and the total cavopulmonary connect (or Fontan completion) [22]. A system incorporating a patient-specific 3D-printed Fontan model has indeed been realised [23].
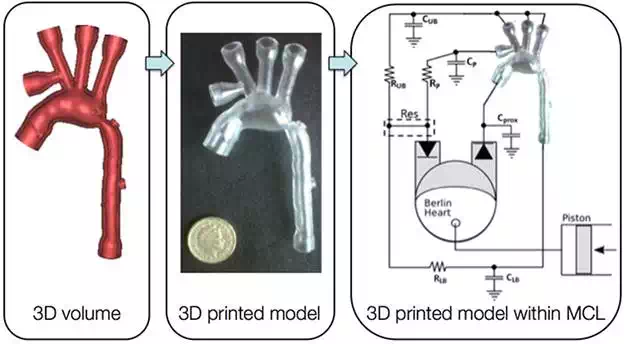
FIGURE 5.
Model of the aortic arch of a baby with hypoplastic left heart syndrome following the Norwood operation and including a visible aortic coarctation. The 3D volume (left) is modified for the purpose of carrying out hydrodynamic experiments, hence including funnelled attachments to the MCL and ports for pressure measurements along the aorta. The volume is 3D printed with rigid resin (centre) and inserted in the MCL (right), which is here represented with its electrical equivalents, including a Berlin Heart® device to simulate the single ventricle.
VISUALISATION STUDIES AND VALIDATION OF COMPUTATIONAL MODELS
An MCL which incorporates 3D-printed anatomical models can be utilised to two additional ends: (a) serving the purpose of validation test beds for computational models and (b) generating detailed information on local fluid dynamics by means of visualisation experiments. In the first case, computational models have been introduced as a powerful resource for generating knowledge in CHD and possibly aiding in the decision-making process [24], but, in order for numerical models to be reliable, they require thorough validation against ‘real world data’ [25] which can be obtained in vitro. In the second case, the MCL can be modified to be compatible with different visualisation techniques, e.g. particle image velocimetry [23] or magnetic resonance imaging, thereby generating detailed visualisation data. A case study of CHD, namely transposition of the great arteries (TGA) repaired with the arterial switch procedure (ASO), was modelled for both purposes [26]. In this study, an MCL was built in order to be compatible with CMR image acquisition, and a 3D patient-specific model was inserted in the MCL for visualisation purposes. The model was reconstructed from CMR data of a patient (16-year-old male) with repaired TGA with ASO and Lecompte manoeuvre, showing typical features of TGA aortic arches (i.e. a dilated aortic root and a gothic aortic arch), thereby representing a representative test bed for studying haemodynamics in this clinical scenario. The model was 3D printed with transparent rigid resin. Visualisation data were acquired with 4D CMR flow, which generates exquisite images of flow streamlines within the volume of interest over the cardiac cycle. An age-matched control model (i.e. no CHD) was included in the study for comparison purposes. Furthermore, the model was replicated in silico in a multi-scale model including the same 3D domain (i.e. TGA or control aortic arch) and a lumped parameter network summarising the remainder of the circulation. Qualitative and quantitative comparison of flow and pressure data was carried out in order to validate the computational model, demonstrating good agreement between the two for both TGA and control scenarios. An example for this modelling paradigm is shown in Figure 6.
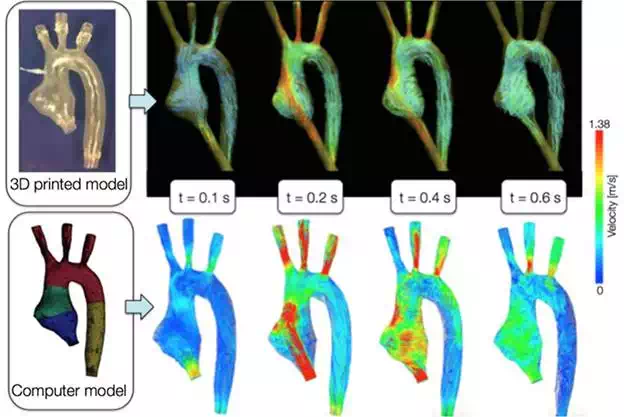
FIGURE 6.
A model of the aortic arch 3D printed for visualization CMR experiments (top) and meshed for computational simulations (bottom). The images show example of flow-velocity streamlines from both CMR and computational fluid dynamics at the same time points through the cardiac cycle, showing good qualitative agreement as well as agreement of velocity magnitudes. Further quantitative comparison was carried out in this case study to show the goodness of the agreement between computational and experimental data (i.e. validation of the computational model).
TESTING DEVICES: THE NEED FOR COMPLIANT 3D MODELS
Experimental models can not only incorporate 3D-printed models but can also be used to test devices, e.g. a stent deployed into the 3D model itself. The system can, as per 4.2, be not only valuable for testing novel devices but also for generating validation data for computational model of the device itself. From a 3D printing perspective, in this case, it is interesting to consider what options are available in terms of 3D printing materials. While for other experiments or other applications and conventional materials such as SLA resins might be appropriate, in the case of deploying a device inside the 3D model, it may be desirable to implement the realistic compliance of blood vessels, allowing the device to adapt well to the anatomical implantation site. With advances in 3D printing technology, models such as silicone are becoming compatible with the printers, thus opening interesting avenues of research. One of the first 3D printing compatible compliant materials was a commercially available compound (TangoPlus FullCure) [27]. A study was carried out to evaluate the range of distensibility that can be implemented by models of varying thickness printed with such materials. The study showed that the material is suitable for implementing the distensibility of different arteries, in a range of thicknesses 0.7–1.5 mm. However, limitations of the materials include its fragility (i.e. tearing under pressure) and cost (more expensive that printing the same model in a rigid resin or nylon). The models for the compliance tests were 3D-printed segments of the descending aorta of a healthy volunteer, approximating a cylinder for ease of testing. Other anatomies were also 3D printed with the compliant compound. For instance, a study was carried out to test the implantation of a PPVI stent (see Section 3.1) in a patient-specific implantation site. By testing the device in a compliant model, it was possible to appreciate the way in which the stent adapted to the shape of the implantation site and deformed according to the anatomy (Figure 7). As per the validation framework (see Section 4.2), the same setting was also reproduced in silico [28].
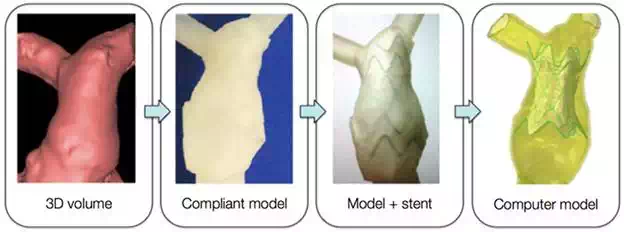
FIGURE 7.
Reconstruction of patient-specific right ventricular outflow tract from CT data (‘3D volume’) which is 3D printed using a compliant rubber-like material (‘compliant model’); a stent is inserted inside the 3D model for testing (‘model + stent’) and additional data can be acquired by replicating the ‘model + stent’ system computationally. Stent diameter at extremities = 40.7 mm.
Nowadays, TangoPlus FullCure is not the only option for 3D printing compliant materials for simulating arterial models. For example, another commercially available compound, namely Heart Print Flex [29], represents a valid material for 3D printing compliant cardiovascular models. Considerations of 3D printing compliant models include the wall thickness, which may represent a limit in terms of the printer resolution and in turn could restrict the range of distensibilities that can be implemented. Robustness of the models would also be desirable if these were to be used for hydrodynamic applications, e.g. testing devices in deformable models under pulsatile flow.
Facilitating doctor-patient communication
Communication between cardiologists/surgeons and patients with CHD and/or families of children with CHD is a delicate issue and an example of communication between an expert and a non-expert subject in which the information being exchanged is both sensitive and complex [30]. Studies have shown that understanding CHD and overall knowledge of the defect can be an issue in both patients, particularly adolescents, and their families [31]. Important information, such as the name of the primary diagnosis, has been shown to be difficult to retain in some instances, which could represent an issue for reporting information to other medical professionals caring for the patient and the patient closer community. Also, knowledge of the defect and overall appreciation of the anatomy can have an impact on lifestyle adjustments, for both the patient and the carer. In this light, improvements in communication with novel tools can be highly desirable. 3D models printed with rapid prototyping technology have been advocated to be potential communication tools; however, evidence in this context is lacking. As part of the translational work at the Centre for Cardiovascular Imaging, models were purposefully manufactured for communicating with patients and families. A questionnaire-based study [32], in particular, was designed to assess parental knowledge of CHD, randomising parents into two groups: a) with 3D model and b) routine consultation without model. Models of a range of CHD were manufactured in white nylon, as a neutral choice to approach the parents. Examples of 3D models from this study are shown in Figure 8. The study provided some interesting findings. It was noted that using 3D models during clinical consultations in the setting of cardiac transition clinic lengthened consultation time by 5 minutes on average, possibly indicating a more thorough explanation. Clinicians rated the models as ‘very useful’ and reported that generally parents interacted well with the models. Parents themselves greatly appreciated the models and commented positively on their features. However, short-term knowledge, quantified by open-end answers but also through the use of diagrams and keywords (Figure 9), did not appear to improve across the two groups. When two blinded cardiologists were shown the parental responses to the questionnaire, they were unable to identify the primary diagnosis of the child in still approximately 40% of the cases. On the contrary, feedback provided insight into some interesting features of the models from the parents’ perspective. Parents reported that medical images (e.g. echocardiography images, often times shown during consultation) are ‘meaningless’, while a 3D model ‘makes it all so much easier for the non-expert to understand’. Parents reported some degree of shock in realising the patient-specific nature of the model (‘[…] seeing the model of my son’s heart was quite a shock’) but understood and appreciated the value of the model for communicating anatomical features of the CHD (‘[…] once I was used to the idea that the model I was looking at was what my son’s heart actually looked like, it was a very useful tool for the doctor to illustrate exactly what was wrong with his heart’).

FIGURE 8.
Samples of models (not to scale) that are 3D printed in white nylon for assessing parental knowledge of CHD in a questionnaire-based study. All models are reconstructed from CMR data.
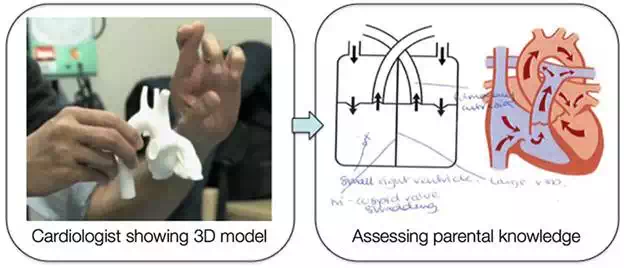
FIGURE 9.
Cardiologists used 3D-printed models in discussing the anatomy and the CHD with the parents and the patients during their consultation. Parental knowledge was assessed before and after the consultation to assess possible improvements in short-term knowledge after having seen and manipulated the 3D model.
This line of work touches on important principles of patients & public involvement and engagement (PPI/E) in research. PPI, according to the INVOLVE national advisory group (part of the National Institute of Health Research), can be referred to as research that is carried out with/by the public, not about/for them, e.g. prioritising research topics, taking part in steering groups, undertaking research or disseminating research findings [33]. The importance of developing PPI is linked to the fact that research stemming from a PPI framework is likely to be more ethical and more relevant for the patients. The area of 3D printing cardiovascular models can be conducive to developing PPI, by actively involving patients’ representatives in the process of improving not only model features or prioritising their use but also the communication around CHD and in turn promote a PPI framework through a true conversation with patients and their families (Figure 10).
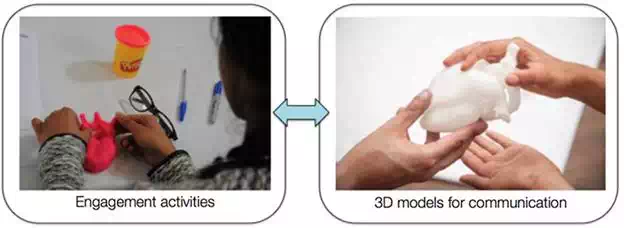
FIGURE 10.
Engagement activities with patients and families can be carried out by a multidisciplinary team exploring concepts such as making a 3D heart (left: patient with CHD making a 3D heart with Play Doh®). Developing a conversation with the public can in turn inform better usage of 3D models and technology for communication purposes. Right image courtesy of Stephen King.
A multidisciplinary approach: incorporating 3D models in an art installation in a clinical setting
As part of the research activities of the Centre and of Great Ormond Street Hospital for Children, interactions with artist in residence Sofie Layton have resulted in an innovative and exciting use and display of 3D-printed models in the hospital/research setting. A multidisciplinary collaboration was established with the artist, developing an arts-and-science approach for the study of some CHD features. In particular, the artist was developing ‘Under the Microscope’, a project supported by the Wellcome Trust to explore how patients and families process medical information and medical language. While also exploring rare disease, Sofie Layton immersed herself in the world of CHD by familiarising with CMR images, features of the anatomy of different defects, running workshops with CHD patients and their parents, developing a conversation with cardiologists and nurses, and also appreciating engineering methods that can play a role in this context, such as computational simulations and 3D-printed models. From an artist’s perspective, 3D printing is a fascinating concept and the exploration of forms that the technology allowed specifically for CHD was the starting point of the collaboration. In the culmination of the project, Sofie Layton realised two installations (exhibited at the Institute of Child Health and Great Ormond Street Hospital for Children, February-April 2016). One of the installations revolves around CHD, including participatory work, a soundscape recounting the journey of a cardiac patient, panels that illustrate the language of CHD (i.e. anatomy, conditions, medications, treatments, narratives), as well as 3D-printed anatomical models (Figure 11).
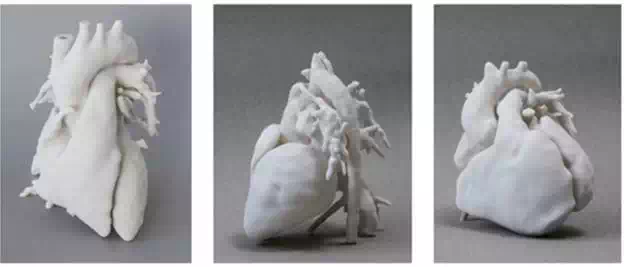
FIGURE 11.
Examples of 3D models realised for Sofie Layton’s ‘Under the Microscope’ art installation, including a normal heart (left), a case of repaired TGA with ASO (centre), a case of repaired tetralogy of Fallot (right). Image courtesy of Stephen King.
In this context, models lend themselves to contribute to this site-specific installation by representing the variety of forms and arrangements that the cardiovascular anatomy can present, but the artist can take the process one step further. By exploring shapes and sizes, some unconventional models are included in the landscape (see Figure 12). A small bronze heart, suspended in a bell jar, is the result of scaling the 3D volume of a normal heart model, 3D printing a mould and casting a precious heart, sparking a reflection on the preciousness of the organ and of the stories and symbols associated with it. Similarly, another model, also 3D prototyped, has been virtually manipulated prior to printing so to resemble a Rubick’s cube, which emerged from a conversation with a patient as a powerful image of the complexity of his heart following multiple repairs of CHD. The models are positioned on a sterile-looking stainless steel table in amongst the other artwork, essentially creating a dialogue between medical conditions and real-life stories. This collaboration is an example of how 3D printing technology allows for a stimulating exploration of possibilities of expression, which is facilitated and promoted by the continuous dialogue between the artist and the engineer, in a sense pushing the boundary of the technology for its medical use. The piece, indeed, has a clinical relevance, as well as relevance for the abovementioned concept of PPI/E. By creating this landscape (including sounds) in a medical/research setting rather than a neutral space, the installation echoes conversations and stories that have taken place within that dimension but enriches them by allowing for one final element to emerge: the human element. It is the artist who takes the responsibility of blending real-life stories in between anatomical models, technical jargon and heart outlines from CMR. This innovative approach presents yet one more use for 3D-printed models and for the possibility of expression offered by this technology.

FIGURE 12.
Installation of 3D models under bell jars, as part of Sofie Layton’s piece ‘Under the Microscope’. While most models have a medical appearance, 3D technology is allowed to manipulate the data and scale it to create, for instance, a small bronze heart (right) which the artist chose to suspend in one of the bell jars. Image courtesy of Stephen King.
Outlook and considerations for future research
Based on a single-centre experience, 3D printing can present several relevant uses for the study and communication around CHD. Such a revolutionary manufacturing technique allows to generate, in a relatively short time and at a relatively affordable cost, patient-specific models, which—as discussed— are particularly relevant when referring to unique anatomical arrangements, as often the case in CHD. Based on our Centre’s experience, as briefly outlined in this chapter, uses range from testing novel devices and appreciating patient suitability for a specific device, providing additional insight into a particular anatomy, allowing for performing parametric studies and validating computational models, as well as representing a medium for implementing PPI/E in this area of medicine. A few considerations are necessary with regard to the future uses of 3D printing for CHD, including
● Image availability: the creation of 3D models is, of course, dependent on the availability of imaging data (CMR, CT) and of 3D datasets within the imaging protocol; this should be taken into account when considering which patients could potentially receive a 3D model or for which cases a 3D model could be created, e.g. for aiding decision-making (i.e. if there is no clinical indication for imaging, then a model will not be available for that case).
● Operators: image segmentation and reconstruction does currently still require a specialised operator, and it can be a time-consuming task depending on the complexity of the defect(s) and imaging quality; while ours is a specialist Centre in CHD and has a team on engineers in situ, other centres may not have the capabilities of handling the data and/or manufacturing the models, which can be a hurdle towards clinical translation;
● Cost: depending on the volume of the part and the material, models can cost in the range of £30–£500. When considering a large volume of models, for potentially translating the technique to the point of even becoming a service, an appropriate cost-effectiveness analysis should be carried out on a large scale, including not only the printing costs but also the man time for image elaboration, which is integral to the process. This element is still lacking.
● Printing time: a full heart model of an adolescent would typically require around 6–7 hours to print (or left to print overnight); however, recent advances on the technology side have led to 3D printers that boast drastically quicker printing times than current technologies. The possibilities of fast printing could be appealing for clinical translation, depending on the cost.
● Efficacy: regardless of the cost, clinical translation of 3D printing models in medicine and in CHD in particular still depends on the demonstration of its efficacy. Considering the rarity of some CHDs, this requires a multi-centre effort. While initiatives such as the NIH 3D Print Exchange (Heart Library, http://3dprint.nih.gov/collections/heart-library) bring together a large number of models, a systematic quantification with statistical evidence of the usefulness of the models in clinical practice is also lacking at present.
● Other applications: other uses of 3D models are currently being explored beyond those mentioned in this chapter, particularly including the use of 3D models of CHD for training purposes (e.g. nurses or students); the use of 3D-printed models for training has been used in other areas of medicine [34] and also, in CHD, in a study that focused on the appreciation of ventricular septal defects in a cohort of medical students [35] suggesting the beneficial use of 3D models for better appreciation of the defect.
● Availability of the technology in situ: it is very rare that a clinical centre would have 3D printing facilities, at the moment; research hospitals would likely have access to the facilities via academic collaborators. This might change in the near future, depending on the development on new machines, possibly including high-definition desktop 3D printers, which are affordable and do not require a specialised dedicated room, depending on the purpose for which the model is required.
● Collaboration: as for any translational effort, collaboration is of paramount importance between different users and between different specialists, in this case particularly between engineers (on the technical side) and clinicians (on the user side). The patients’ perspective is also important, especially for using models for communication purposes, and a PPI/E framework should be advocated for such applications.