Colour Image Reproduction for 3D Printing Facial Prosthese
Maxillofacial prosthetics or anaplastology refers to the specialty that designs and manufactures prostheses used to replace part or all of any stomatognathic and/or craniofacial structure. The process provides descriptive evidence of the prosthesis, including location, retention, support, time, materials, and form. It is both an art and a science of cosmetics, anatomy and functional reconstruction, that is achieved by means of artificial substitutes of head and neck structures that are missing or defective. It is the branch of dentistry that rehabilitates intra‐ and extra‐oral deformities [1]. Extensive tissue loss involving facial (or indeed any other body structure), on many occasions, cannot be corrected surgically due to a lack of sufficient or adequate donor tissue that may be required for the surgical repair and reconstruction. Furthermore, the patient's age and general condition may not permit extensive surgical procedures or allow for the morbidity often associated with protracted courses of reconstructive surgery and recovery [2]. Additionally, the final outcome can often be aesthetically and functionally compromised. In such cases, defects may be replaced artificially with the provision of facial prostheses to provide functional rehabilitation and aesthetic improvements. Often there is an associated improvement in social, emotional status and overall quality of life [3].
Traditional methods of prosthesis production are well established and are used even today. These include taking an impression, manufacturing a cast and ultimately hand crafting a prosthesis in a silicone based or similar material. The provision of prostheses in this manner has provided considerable comfort and support to many patients over many years, and allowed them to continue with normal day‐to‐day activities and enhance their social interaction [4]. Despite the advantages this method can provide, its application has shown some limitations and shortcomings. These are primarily related to the processing strategy, technical expertise required, time, effort, cost and retention problems. Furthermore, there are durability issues due to material degradation and colour fade after a relatively short period of service because of general wear and tear and exposure to ultraviolet radiation. For these reasons, facial prostheses require renewing and periodic replacement, which is a costly and time‐intensive process, which places a burden on both patients and prosthodontists alike [3].
In the last decade, additive manufacturing technology, including three‐dimensional (3D) printing, has advanced dramatically. Colour 3D printing has also evolved to produce full spectrum coloured solid objects utilising a range of materials [5, 6]. With the evolution of various 3D imaging techniques, accurate acquisition and transformation of target object geometric data into 3D digital models can be achieved. By combining the 3D image capture and printing techniques, there is huge potential to achieve ‘What You See Is What You Get’ processing. More importantly, it has the ability to directly interconnect with advanced manufacturing techniques, allowing customisation with high accuracy, resulting in savings of both time and costs [7]. It has been extensively utilised in rapid prototyping [7], successfully applied in medical sciences [8, 9], and is gaining popularity in multidisciplinary applications [10–12]. For medicine, captured digital 3D models have great accuracy and have been effectively used for facial disfigurement diagnosis, surgical planning and assessing treatment outcomes for several years [13, 14]. Additionally, there is the potential to develop this automatic additive manufacture technology for facial prosthetics.
Compared with conventional image capturing technology, image processing between 3D image devices has much more complicated working processes. For 3D printing, the quality of 3D printed objects is not only affected by the printing itself including binder/substrate interaction and printer resolution, but also the printing material and any post‐processing or finishing stages [15]. Therefore, without a specific protocol, 3D objects can often be produced with poor reliability, accuracy and quality. Moreover, in terms of 3D image reproduction, image processing methods to transform 3D images from a 3D camera to a 3D printer are far less well developed than existing processes that use 2D technology. Furthermore, accurate colour reproduction for facial prostheses is highly desired and the quality of skin colour reproduction can affect the overall quality of the facial prostheses significantly. Therefore, accurate colour management processes are not only essential, but also needs to run in conjunction with the specific 3D manufacturing processes used.
In recent times, new and innovative methods for manufacturing facial soft tissue prostheses that prioritises accurate 3D colour image reproduction have been developed and a framework and protocol for specific 3D processing designed [16–18]. Additionally, colour management processes have been developed and successfully applied to 3D imaging devices and manufacturing processes.
Protocol of colour image reproduction
Based on the steps shown in Figure 1, a 3D colour image reproduction protocol has been developed for the automated 3D printing of facial prostheses. The first step involves 3D scanning of the face using a 3 pod 3dMD photogrammetry system (3dMD, Atlanta, GA, USA). The system captures both 3D topography and colour information of the scanned surface in controlled illumination and viewing conditions. The resulting mesh data from the scanner often has errors in geometry and colour and therefore requires further editing before it can be sent to the printer. Using a combination of software suites, for example Magics (Materialise, Leuven, Belgium), the raw scanned data can be modified and corrected by removing noisy polygons, along with colour adjustment of areas with specular highlights or other inaccuracies. In order to add realism, the next step involves the addition of fine texture (e.g. pores, wrinkles) over the 3D mesh using high‐field mapping. Finally, thickness is added to the mesh data in order to get a solid printable model.
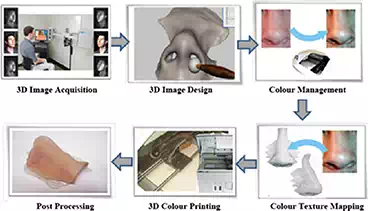
FIGURE 1.
3D image reproduction protocol.
As with the surface topographic information, the colour images from the 3dMD camera system may also require further processing before they can be overlaid on the 3D mesh prior to final colour printing. This primarily involves colour management of the 2D colour image from the camera RGB to printer RGB for each pixel using specific camera and printer colour profiles respectively. For this specific task, the colour profiles used were developed using both conventional colorimetric and spectral‐based reproduction methods [19, 20]. When the colour management is finalised, surface texture mapping is conducted to map the newly generated colour image onto the manipulated 3D model. The penultimate step involves 3D colour printing to produce the 3D model using the 3D printing system, and then, finally as a post‐processing step, the strength and flexibility of the printed model are improved by infiltrating it with medical grade silicone.
3D image acquisition
3D facial data can be obtained using a variety of different techniques. CT and MRI scans have been used for the RP of internal body organs and structures as well as facial prosthesis prototyping. These techniques have an advantage over external body 3D scanning as they can be used for generating patient specific 3D models of internal body parts or organs, etc. However, due to their lower resolution, they are unable to capture fine textural details like pores and wrinkles on the surface of the body. Furthermore, data capture is undertaken in supine positions and thus can affect the accuracy of captured data in that the positional detail is not truly reflective of that in a natural upright repost position. Finally, there is no ability to capture colour data using these modalities.
Compared to CT and MRI, 3D photogrammetry is becoming more popular due to the expediency of the data capture, lack of exposure to ionising radiation, ability to capture data in a prone position, and relatively easy storage, transfer and utilisation of the data. Furthermore, the cost of such systems is relatively affordable. Active 3D scanning techniques like laser scanning [21], Kinect [22], structured light [23] and speckle projection stereo [24] have also been used previously to obtain 3D scanned data for manufacturing of facial prosthetics. Although the image acquisition and 3D reconstruction techniques are different using these methods, the outputs produced are similar in terms of the data produced and they all produce 3D mesh data and colour information for the scanned geometry.
Typically surface scanners, including the 3dMD scanner, are based on the speckle projection technique and was used successfully in this project. This system is based on stereo photogrammetry and calculates stereo correspondence by projecting infrared speckle patterns over the target surface to then create a 3D depth map of the scanned surface. It consists of several machine vision cameras and infrared speckle projectors combined with a flash system to acquire texture and 3D topographic information simultaneously. These are collectively known as pods. The process then merges all the viewpoint data from each pod to create the final 3D polygon mesh with the colour images then laid over the 3D mesh to add colour, texture and appearance. The resulting mesh can then be saved as an .OBJ file for processing and editing purposes. An example of this scanned data is shown in Figure 2.
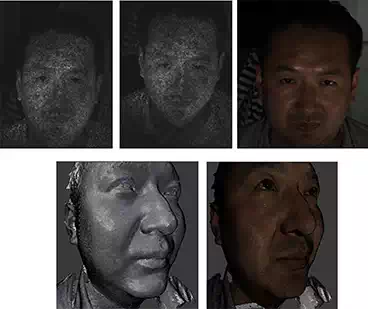
FIGURE 2.
(a)–(c). a) Speckle projection images and texture bitmap captured from a single pod. (b) 3D mesh created 3 using all viewpoint data. (c) The 2D bitmap image overlaid over 3D mesh to add colour.
To ensure sufficient quality images, protocols can be developed to aid data capture. These can include—capturing images in a blackout facility, minimising patient movement, employ consistent peripheral lighting protocols and following the camera manufacturers recommended protocol for image capture, including geometric and colour calibrations immediately prior to imaging. When capturing images to use in the 3D printing of facial prostheses, patients should be asked to remain motionless during the image capturing process in order to avoid any motion artefacts. If the patient has already had surgery to remove the affected facial part, they will often have precision attachments retaining existing prostheses. In cases such as these, due to the limitations of data capture for these attachment—small componentry, shiny surfaces, obscured by anatomical features including prominences, undercuts and recesses, acrylic bosses (described below) can be used to ensure the camera captures the exact location of any precision attachments being used. Ideally, the patient should also be maintained a neutral pose during imaging.
3D image design
Raw data obtained from 3D camera systems often require further processing prior to 3D printing. Depending on the anatomical location of the prosthesis, mesh editing can consist of the following steps.
Data preparation
CAD generation of the missing facial part can take various forms. Data capture of unaffected areas of the face can be undertaken and images ‘mirrored’ in order to virtually replace those affected or missing. This may be suitable for missing ears or orbital areas where there are usually bilateral structures. However, this may not be appropriate or possible for single or isolated structures including nasal structures or where surgery has already been undertaken to remove the affected part. Alternatively, open‐source CAD databases are now increasingly available—www.turbosquid.com—and these can offer CAD users direct links to downloadable content. These may include non‐specific facial shapes covering a wide range of anatomical form, from those considered ‘generic’ to those with interesting or characteristic features. Although easily accessible, there are some issues with these sources. Although geometrically accurate, the peripheral area can be quite variable and not suited to cover the affected areas in specific patients. Additionally, the surface detail can be highly faceted and unsuitable for direct modelling. However, these files can provided good starting points for CAD design and allow adaptation to enable conformation to the affected area. Various software can be used to alter theses captured or acquired data files including 3‐Matic (Materialise, Leuven, Belgium). These can then be used to alter the surface detail and to refine the geometry in order to provide individual and bespoke characteristics for the missing facial part (Figure 3).

FIGURE 3.
Image detailing manipulation of the CAD prosthesis to refine the shape and fit of the final part (Approx. part Dim: 40 × 24 × 25 mm).
Data manipulation
The acquired and adjusted model can then be blended into the affected area to create a smooth margin that will contact the facial tissues. Furthermore, CAD prostheses occasionally require hollowing and thinning until the prosthesis is between 2 and 3 mm thick and this can again be undertaken with various software packages. Finally, the model is then trimmed to remove all unnecessary data prior to printing. As previously indicated, information for attachments can then be imported and merged with the prepared CAD prosthesis and be precisely aligned to produce a good retentive element and fit.
Precision attachment design
Often facial prostheses are retained using precision attachments including osseointegrated implant retained magnets, bars and clips. In these situations, external markers, or bosses, are used to identify the position, angulation and orientation of any attachments that need to be incorporated into the data incorporated in to the process. Their position can then be translated through the design and manufacturing process into the final prosthesis (Figure 4).
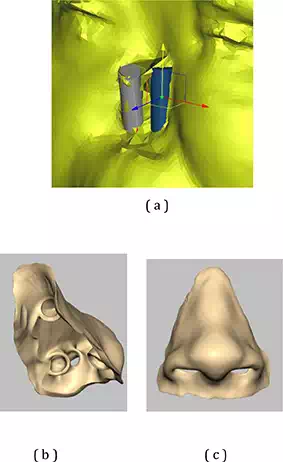
FIGURE 4.
(a) Images illustrating the use of external markers, or bosses, to detail the position of precision attachments to aid retention of the prosthesis. (b) Translation of the geometric position of the attachment points for the precision attachments within the prosthesis (Approx. part Dim: 40 × 24 × 25 mm). (c) Checking of CAD design to check no interference of surface geometry caused by incorporation of precision attachments.
Data detailing
Natural orifices such as nasal apertures and auditory canals must be designed to ensure that the prosthetic has correct anatomical form and be modelled in a way that will allow for appropriate function if needed. For the nose, it will allow for the passage of air during respiration whilst for the ear, although external form may be missing, it will allow non‐impeded hearing via direct access to the external auditory meatus (canal). Similar considerations can be made when designing orbital prostheses as the housing of an artificial glass or acrylic globe will be required within the palpebral fissure (eye lids). In some instances, it should be remembered that the provision of attachments may impinge on these design features and so optimal modelling and detailing must be undertaken to camouflage these issues.
Design finalisation
Once the final model has been produced, additional details need to be added in order to produce a satisfactory prosthesis. Final details including the incorporation of peripheral extensions, feathered edges, any necessary strengthening buttresses and the smoothing of seams and joins on the model's inner surface can all be undertaken prior to printing. The colour calibration image is then also applied to the whole model prior to production.
Colour management
Due to the different ways in which colour communication between 3D image capture and 3D image printing is utilised, there are often significant discrepancies in colour between the printed and original objects when using this type of manufacturing process. Conventional colour image reproduction techniques based on CIE colorimetry have been used for more than 80 years and perform very well in transforming colour images from one digital media to another under various viewing conditions [25]. However, the application of conventional colour image reproduction techniques for 3D printing technology is not as straightforward. With this protocol, 3D colour objects can be split into a monochromatic 3D objects and a 2D colour images. With this in mind, a conventional colour reproduction technique can be applied to transform the 2D colour image from camera RGB to the corresponding printer RGB through human colour appearance attributes. To achieve an accurate colour reproduction through 3D imaging devices, specific colour profiles need to be developed in order to link the colour system of a specific device to the human visual system [26].
DEVELOPMENT OF COLOUR PROFILES FOR 3D IMAGE DEVICES
To truly reproduce colour from a 3D camera to 3D printer, both a camera colour profile and a printer colour profile need to be developed to connect camera RGB and printer RGB with human eye response (CIE XYZ tristimulus values [27]). Variations in skin colour and tones are considerable [28], and to try and incorporate the whole spectrum of skin colours available for different human populations templates such as the digital Macbeth ColorCheckerDC charts (X-Rite Inc., Grand Rapids, MI, USA) can be used to provide numerous training colours (see Figure 5a). Utilising this method, a 2D colour chart can be converted to a 3D model with dimensions of 200 (l) × 150 (w) × 3 (h) with the colours desired and printed using a 3D printer such as a Z Corp Z510 colour printer. These can then be used as your testing colours (Figure 5b). Subsequently, the CIE XYZ tristimulus values for each training colour produced in the printed colour chart can be obtained by taking colour measurements using a spectrophotometer such as a Minolta CM‐2600d (Konica Minolta Inc., Tokyo, Japan). During measurements, standard viewing conditions should be applied such as a viewing geometry of d/8 (diffuse illumination, 8‐degree viewing), with specular component included and aperture sizes consistently set to a defined diameter—3 mm. The illuminant must also be consistent and ideally of an industry standard including setting to CIE standard D65 to simulate skin colour in daylight conditions and CIE 1931 standard observer [27].

FIGURE 5.
3D models of a) training and b) testing chart.
Based on printer RGB and CIE XYZ tristimulus values for the training colours, a printer colour profile can be developed using a third‐order polynomial regression model [28]. A camera colour profile can also be produced utilising the same chart. Colour images are captured by the 3dMD camera system and the camera RGB for the number of training colours used identified. Then, based on these camera RGB and CIE XYZ tristimulus values, a camera colour profile can be developed using a second‐order polynomial regression [29]. Using this method, for each pixel of image, camera RGB is first transformed to CIE XYZ tristimulus values and then transform back into printer RGB.
Evaluation of colour reproduction
To evaluate colour reproduction for the human face, a colour test chart first needs to be designed. This can be undertaken using 14 predetermined human skin colours, including four Caucasian, two Chinese, two Asian, four African and two Caribbean skin shades (see Figure 5b) [30]. A 3D colour chart must then be generated using the colour printer to be used (Z Corp Z510), with defined and consistent dimensions. After post-processing in the same way any final prosthesis would undergo, this chart is referred to as the original colour chart.
Colour reproduction can then be evaluated using two reproduction charts that must be produced using two different 3D colour image reproduction systems. When the first chart is produced, the colour image for the original chart must be captured using the 3dMD camera system and then processed with only minor corrections in 3D geometry before it is sent to the Z Corp Z510 printer for 3D printing. This printed colour chart can then be referred to as the first reproduction (Chart 1). For the second processing, it can be conducted following the proposed 3D colour image reproduction process. This printed chart can then be referred to as the second reproduction chart (Chart 2).
To assess the performance of the colour reproduction, CIE XYZ tristimulus values for each colour patch within each colour chart must be measured using a spectrophotometer (Konica Minolta cm‐2600d). Colour difference between the original chart and each of the two reproduction charts for each of the 14 testing colours under CIE illuminant D65 should be calculated using a CIELAB colour difference formula [31]. The mean, maximum, minimum and standard deviation for the colour difference can be recorded and tabulated. Examples of these values can be seen in Table 1. If undertaken correctly, this method will demonstrate that a significant improvement in colour reproduction can be achieved using 3D colour image reproduction systems. For its successful application in the production of facial soft tissue prostheses, an acceptable colour difference for the 3D printed objects is approximately 3–4 ΔE*ab[32].
|
CIE ΔE*ab |
Mean |
Max |
Min |
SD |
|
Org vs. Rep1 |
20.8 |
27.8 |
8.0 |
5.5 |
|
Org vs. Rep2 |
4.5 |
11.1 |
2.5 |
2.3 |
TABLE 1.
Examples of colour difference between original (Org) colour chart and reproduction (Rep) colour charts.
Colour texture mapping
Many 3D photogrammetry systems can give the illusion of texture by wrapping the 2D image over the 3D surface. This wrapped texture does not actually produce fine wrinkles, pores or blemishes on the surface of the skin and hence cannot be reproduced within the rapid prototyping process.
Figure 6a demonstrates a side‐by‐side view of a 3D polygon mesh and the 2D bitmap image captured by a 3D camera system (3dMD System). It can be seen from the image that the 3D mesh does not actually contain fine details including pores and wrinkles, which are clearly visible in the 2D bitmap. Each polygon in the 3D mesh is linked to a particular region in the 2D bitmap. Figure 6b shows highlighted polygons in the 3D mesh and the region used from the 2D bitmap to overlay colour onto a monochromatic polygon.
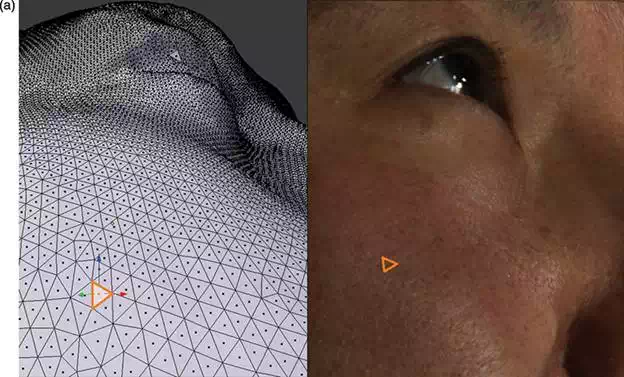
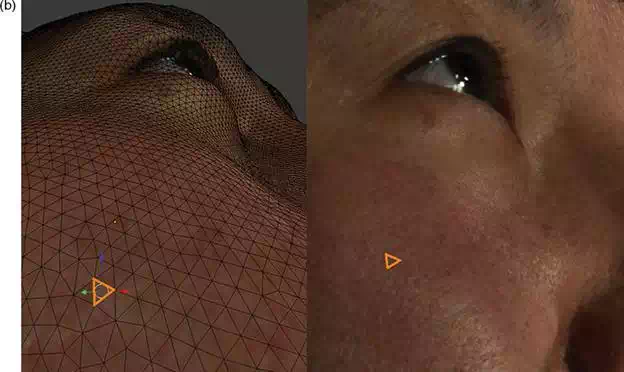
FIGURE 6.
(a, b). Images demonstrating a 3D polygon mesh and the 2D bitmap image captured by a 3D camera system.
To enhance realism and improve the characterisation of the patient's skin, various techniques have been developed. One such method includes incorporating surface details such as pores, wrinkles and fine lines into the 3D model. Height‐field mapping (also known as bump mapping) within the CAD design process can be used to translate the texture reference image onto a geometric pattern. Height‐field mapping is a method of translating fine 2D images onto 3D geometric virtual models. This is based on white (high) and black (low) greyscale texture reference mapping as detailed above, and can be applied to map representative texturing to the appropriate areas of the facial model. These techniques can not only use patient specific data from adjacent facial anatomy/topography but also, using pre‐treatment 2D photographs of the same area. The latter allows for manually adding realistic skin textures to the prosthetic model surface in cases where texture from other parts of the missing face are either inappropriate or not consistent or representative of the area to be replaced. Based on the grey level intensity (from white to black), computer software can control the depth of imperfections over a skin surface. An original skin depth map is shown in Figure 7 (a) and can be used to add texture over a flat surface. Surface topography changes according to the grey level intensity and the positioning of individual pores and wrinkles is shown in (b). The resultant mesh can be 3D printed, producing a skin‐like texture over a flat surface (c).

FIGURE 7.
(a) Depth map of skin showing pores and fine wrinkles as dark areas. (b) Software‐induced texture mapping over a flat surface using the depth map from (a). (c) 3D printed surface with pores and wrinkles clearly visible on the surface (Approx. part Dim: 38 × 38 × 3 mm).
Given the flexibility of such software, texture can be mapped not only onto flat surfaces but also over complex 3D shapes. An example of this texture mapping over a nose model with varying pore depths is show in Figure 8.
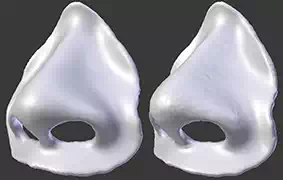
FIGURE 8.
Illustrations detailing texture mapping. (Approx. part Dim: 70 × 61 × 29 mm).
However, the detail provided in the final prosthesis is dependent not only on the resolution of 3D data obtained but also the resolution of the 3D printer and characteristics of the powder and binder type used within the process. The use of course powder in the printing process will reduce the detail of the texture derived from the height‐field mapping even though such detail can be mapped within the CAD process. In contrast, using finer powder will enable the addition of very fine details over the printed prosthesis.
3D colour printing
Full colour 3D printing is considered advanced technology with different 3D colour printing technologies continually being developed and evolving. One common full colour 3D printing technology is 3DPTM printing, also known as powder–binder printing. Developed at Massachusetts Institute of Technology [33] and licensed to Z Corporation and 3D Systems, the process itself is based on inkjet printing, with the powder being deposited in consecutive layers, which are then selectively joined by ink‐jetting with coloured binder. Three (CMY) or four (CMYK) coloured binders together with a clear binder are mixed to print powder material in a full colour spectrum, layer by layer. After 3D printing, post‐processing, including the removal of excessive unused powder and infiltration, often needs to be conducted in order to produce the final model (Figure 10). The powders can be made of different kinds of materials. Gypsum is primarily used in combination with plastic powder. However, starch, ceramic, glass and other powdered materials can also be processed as well. For manufacturing facial prostheses, 3D printers including the Z Corp Z510 3D printer (3D Systems Inc., Rock Hill, SC, USA) can be used to print colour into biocompatible starch powder. Post‐printing processing is then required. Infiltrating with suitable elastomeric polymer can then be undertaken to produce a flexible, lightweight and lifelike soft tissue prosthesis. More recently there has been the development of other elastomeric 3D printing processes including direct deposition and filament printing. However, their main drawback is the limited spectrum of colour they can print in.
Infiltration base design
The printing process itself will produce a highly accurate solid model of the missing facial part and consists of printed powder and skin coloured binder. Given the resultant structure post‐printing processing is required to infiltrate the model with a suitable material with properties that will lend itself to the role required—light, flexible and durable in nature [34]. Due to the post‐printing processing needed for direct prosthesis printing, an infiltration base modelled from the affected and adjacent area must be generated (Figure 9). The site of the affected area is imported into the process as a single surface using a suitable CAD software programme. Then using the final prosthesis as a guide, the infiltration base can be trimmed to support the prosthesis and any peripheral extension required in order to define the contact point or provide a feathered edge for final fitting. Each requirement of the prosthesis can be developed within the support with the exact nature of the periphery dependent on the type of facial part to be replaced and the characteristics of the surrounding tissue. Smooth peripheral surfaces will be more suited to feathered edges whilst well‐demarcated wrinkles, or surgical margins will be more suited to a well‐defined edge for closer fitting. Final design features in the infiltration base will depend on the geometry of the missing facial part, but drainage holes and reservoirs may be required in order to provide adequate support and infiltration.

FIGURE 9.
Illustrations demonstrating the design and production of an infiltration bed to support the prosthesis during infiltration with a suitable material (Approx. part Dim: 52 × 36 × 25 mm).
Manufacturing
Following CAD manipulation of the model and design of the final prosthesis, data can be converted to .zpr files for exporting to the printer. Again this can be undertaken using suitable software. Using layered production with biocompatible powder and coloured binder, the prosthesis can be printed ready for any post‐processing including infiltration with a suitable elastomeric polymer. In many cases, the resultant printed model is required to rest for a period of time to allow complete drying of the binder and gentle removal of excess powder allows for accurate post‐processing. As detailed previously, it may well be that for large models that have been designed to replace significant portions of facial tissue an infiltration base is required to prevent distortion or sagging during this process. This can be manufactured separately using any suitable hard materials including acrylic, plastic or even metal either by printing or milling.
Prosthesis infiltration
3D printing produces models with excess powder intimately associated with the final structure. The resultant powder has to be gently removed prior to infiltration with a suitable material. The prosthesis can then be immersed into the infiltrant either with or without the infiltration base and a period of time allowed for complete saturation. This process will be dependent on the thickness of the printed model and viscosity and setting characteristics of the infiltrant. All will have to be evaluated prior to production of the definitive prostheses. Ideally, materials with characteristics and properties close to those used in existing production methods should be utilised in order to make a comparable prosthesis. Normally, the materials employed would be either silicone, acrylic or polyvinyl in nature. Given the variability in the characteristics of these materials extended periods of immersion or infiltration under pressure may have to be considered. Following this process, excess infiltrant needs to be removed from key areas such as the apertures, orifices and attachment housings, and then allowed to fully cure and dry. This process normally takes approximately 24 h.

FIGURE 10.
Photograph of a 3D printed nasal prosthesis infiltrated with a compatible medical grade silicone infiltrate (Approx. part Dim: 40 × 24 × 25 mm).
Final preparations for patient
Following production of the prosthesis, it can be delivered to the anaplastologist for final fitting. Given the nature of the manufactured periphery and infiltration with a comparable material, adjustments can be made to both the peripheral fitting surface and colour in order to achieve an exact fit and colour match in normal repose and function. In addition to these changes, attachment components may be secured into place within the prosthesis using appropriate adhesives. Finally, minor changes can also be made to the texture and surface appearance with the addition of mattifying agents or external colourings. The latter will allow for a more natural finish. The prosthesis can then be fitted to the patient. Figure 11 demonstrates a 3D printed nasal prosthesis retained by magnet attachments. Using this contactless approach, production and final delivery were achieved within 48 h. Given that any single print can produce up to 60–80 prostheses in a single run, the relative time required to produce facial prostheses for multiple patients can be reduced significantly.

FIGURE 11.
Clinical photograph shows the fitting of a 3D printed nasal prosthesis retained by magnet attachments.
Discussion and conclusion
In this chapter, it can be demonstrated that using modern technology and applying some of the traditional methods of the maxillofacial anaplastologist, it is technically feasible to rapidly and directly manufacture realistic soft tissue prostheses using 3D printing. Using available 3D imaging techniques, which are more accurate and convenient than taking impressions, and less harmful to the patient than CT or laser imaging, it can be shown that it is possible to generate a precise life like 3D model of a traumatised or defective area. Furthermore, by incorporating attachments, a prosthesis of exceptional fit and retention can be produced.
To achieve a lifelike and naturally looking prosthesis, any method of 3D printing would also have to incorporate accurate colour management processes, which converts patient's skin tone into a machine‐readable format for 3D printing, and provide an accurate intrinsically coloured prosthesis that matches the patient's own skin colour. Furthermore, if suitable infiltration materials are utilised then extrinsic colouring can be added to the prosthesis, either through a coloured infiltrant or painted on by the prosthetist. In addition to the colour management, it is possible to generate a two‐part texture design workflow that allows production to accurately match the patient's original features. Using automatic height‐field mapping and manual carving to enhance the features, it is possible to generate a prosthesis that resembles the patient's original morphology and skin texture. Given the materials that can be used to print such models consideration must be given to the accuracy that can be achieved, not only in terms of surface texture, but also optimisation of the infiltration protocols. These will inevitably improve the production process and the overall finished look.
To enhance the peripheral fit of the prosthesis, consideration must also be given to the site of fitting and protocols developed that will allow the production of a prosthesis with a durable seal and thin feathered edges or well‐defined edges where appropriate. The latter points may be determined by the condition of the existing site, surgery the patient has undergone or the preference of the prosthetist. Given the accuracy of the process and the flexibility to produce either type of periphery, the protocols developed would be suitable for both adhesive or attachment retained prostheses.
There are several significant advantages to the process described in this chapter. By printing the prosthesis directly using biocompatible materials, several steps can be eliminated from the traditional process, including impression taking, mould making, setting the prosthesis in silicon and intermediate fitting steps. Current methods require two to four patient visits over several weeks and significant man hours to produce the final prosthesis. Replacements must use existing moulds or the process must be restarted, and given that old moulds may not be accurate due to changes in disease state or other patient factors, it may not be appropriate to use these for replicating the prostheses. Furthermore, the method described is contactless apart from the final fitting of the prosthesis. As a result, the patient experiences minimal discomfort and inconvenience and data capture is quicker than traditional methods. Furthermore, it enables the prosthetist to store this data electronically for future use and record keeping. Using this digital process, the imaging and colour reference appointment takes approximately 10–15 min. Additionally, the production time is significantly reduced to approximately 48–72 h between imaging and fitting of the finished prosthesis, and as detailed, this process has the potential to produce multiple parts (60–80) in the same timescale and thus reduce the relative production times for each prosthesis significantly. The process is only limited by the CAD input (i.e. image processing and model design/manipulation) although the process is also largely automated. CAD programs can either be used separately, or integrated into one bespoke software that seamlessly passes the model between programs. The only human intervention occurs at the CAD input, design and post‐processing infiltrant stages.
One other benefit of developing and using this technology is the significant cost benefits. The average cost to the health care system to produce a soft tissue prostheses in the UK using traditional methods is approximately £2000–£6000, and the cost remains largely the same for each replacements prosthesis. The per‐unit cost of 3D printed parts with attachments is significantly reduced due to the reduction in labour costs as well as the numbers that can be produced at any one time. Given that the average prosthesis has a lifetime of 1–2 years, and there is an ever more aging population, the long‐term time and cost savings would be significant using this new technology.
However, there are some limitations to this methodology. The process would be dependent on practitioners acquiring new skills, namely software and CAD usage, and this again will be highly specialised. However, in recent years, this technology has been available for conventional hard tissue and dental prostheses, for example, custom‐made dental crowns, bridges, implant abutments and various other hard tissue prostheses. Given that the software associated with these developments has been widely accepted and is considered user friendly and intuitive, the introduction of such technology for soft tissue prostheses should not be difficult. Another consideration may be the limited availability of virtual CAD models that may be required if existing patient data did not exist. However, these are becoming more available and given that once patients have had parts made existing electronic data can also be used for repeat prostheses for the same patient or adapted for new patients. Another limitation may be the initial start‐up costs, which are not insignificant. At present, equipment costs are high, however, with the advancement of new printing techniques and the emergence of numerous manufacturers in the market place, costs are dropping significantly. Furthermore, collaborative or ‘hub and spoke’ arrangements may mean that the data capture and manipulation of missing parts could be undertaken at a local/regional level, whilst the manufacturing process could be centralised to a few specialist production centres. Given that the data will be stored electronically, electronic communications are largely effortless, and similar protocols are seen with other manufacturing industries, this should be easily achievable.
In conclusion, the utilisation of modern manufacturing technologies including 3D printing can provide a quality product quickly and at a significantly reduced cost, labour and patient inconvenience. As detailed, this is a viable method for manufacturing prosthesis using commercially available equipment and software and could easily be implemented clinically.