Three
Mile Island Nuclear Accident

The Three
Mile Island Nuclear Accident was a partial core meltdown in Unit 2 (a
pressurized water reactor manufactured by Babcock & Wilcox) of the Three
Mile Island Nuclear Generating Station in Dauphin County, Pennsylvania near
Harrisburg, United States in 1979. The plant was owned and operated by General
Public Utilities and the Metropolitan Edison Co. It is the most significant
accident in the history of the American commercial nuclear power generating
industry, resulting in the release of up to 481 PBq (13 million curies) of
radioactive gases, but less than 740 GBq (20 curies) of the particularly
dangerous iodine-131.
The Three
Mile Island Nuclear Accident began at 4 a.m. on Wednesday, March 28,
1979, with failures in the non-nuclear secondary system, followed by a
stuck-open pilot-operated relief valve (PORV) in the primary system, which
allowed large amounts of nuclear reactor coolant to escape. The mechanical
failures were compounded by the initial failure of plant operators to recognize
the situation as a loss-of-coolant accident due to inadequate training and
human factors, such as human-computer interaction design oversights relating to
ambiguous control room indicators in the power plant's user interface. The
scope and complexity of the accident became clear over the course of five days,
as employees of Metropolitan Edison (Met Ed, the utility operating the plant),
Pennsylvania state officials, and members of the U.S. Nuclear Regulatory
Commission (NRC) tried to understand the problem, communicate the situation to
the press and local community, decide whether the accident required an
emergency evacuation, and ultimately end the crisis.
In
the end, the reactor was brought under control, although full details of the
accident were not discovered until much later, following extensive
investigations by both a presidential commission and the NRC. The Kemeny
Commission Report concluded that "there will either be no case of cancer
or the number of cases will be so small that it will never be possible to detect
them. The same conclusion applies to the other possible health
effects."Several epidemiological studies in the years since the accident
have supported the conclusion that radiation releases from the accident had no
perceptible effect on cancer incidence in residents near the plant, though
these findings have been contested by one team of researchers.
Public
reaction to the event was probably influenced by The China Syndrome,
a movie which had recently been released and which depicts an accident at a
nuclear reactor. Communications from officials during the initial phases of the
accident were felt to be confusing. The accident crystallized anti-nuclear
safety concerns among activists and the general public, resulted in new
regulations for the nuclear industry, and has been cited as a contributor to
the decline of new reactor construction that was already underway in the 1970s.
Three Mile Island Nuclear Accident: Stuck valve
In
the nighttime hours preceding the incident, the TMI-2 reactor was running at
97% of full power, while the companion TMI-1 reactor was shut down for
refueling. The chain of events leading to the partial core meltdown began at 4
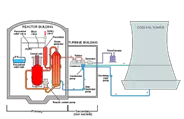
a.m. EST on March 28, 1979, in TMI-2's secondary loop, one of the three main
water/steam loops in a pressurized water reactor. As a result of mechanical or
electrical failure, the pumps in the condensate polishing system stopped
running, followed immediately by the main feedwater pumps. This automatically
triggered the turbine to shut down and the reactor to scram: control rods were
inserted into the core to control the rate of fission. But the reactor
continued to generate decay heat, and because steam was no longer being used by
the turbine due to the turbine trip, the steam generators no longer removed
that heat from the reactor.
Once
the primary feedwater pump system failed, three auxiliary pumps activated
automatically. However, because the valves had been closed for routine
maintenance, the system was unable to pump any water. The closure of these
valves was a violation of a key NRC rule, according to which the reactor must
be shut down if all auxiliary feed pumps are closed for maintenance. This
failure was later singled out by NRC officials as a key one, without which the
course of events would have been very different. The pumps were activated
manually eight minutes later, and manually deactivated between 1 and 2 hours
later, as per procedure, due to excessive vibration in the pumps.
Due
to the loss of heat removal from the primary loop and the failure of the
auxiliary system to activate, the primary side pressure began to increase,
triggering the pilot-operated relief valve (PORV) at the top of the pressurizer
to open automatically. The PORV should have closed again when the excess
pressure had been released and electric power to the solenoid of the pilot was
automatically cut, but instead the main relief valve stuck open due to a
mechanical fault. The open valve permitted coolant water to escape from the
primary system, and was the principal mechanical cause of the crisis that
followed.
Three Mile Island Nuclear Accident: Human factors – confusion
over valve status
Critical
human factors problems were revealed in the investigation about the user
interface engineering of the reactor control system's user interface. A lamp in
the control room, designed to illuminate when electric power was applied to the
solenoid that operated the pilot valve of the PORV, went out, as intended, when
the power was removed. This was incorrectly interpreted by the operators as
meaning that the main relief valve was closed, when in reality it only
indicated that power had been removed from the solenoid, not the actual
position of the pilot valve or the main relief valve. Because this indicator
was not designed to unambiguously indicate the actual position of the main
relief valve, the operators did not correctly diagnose the problem for several
hours.
The
design of the PORV indicator light was fundamentally flawed, because it implied
that the PORV was shut when it went dark. When everything was operating
correctly this was true, and the operators became habituated to rely on it.
However, when things went wrong and the main relief valve stuck open, the dark
lamp was actually misleading the operators by implying that the valve was shut.
This caused the operators considerable confusion, because the pressure,
temperature and levels in the primary circuit, so far as they could observe
them via their instruments, were not behaving as they would have done if the
PORV was shut — which they were convinced it was. This confusion contributed to
the severity of the accident: because the operators were unable to break out of
a cycle of assumptions which conflicted with what their instruments were
telling them. It was not until a fresh shift came in who did not have the
mind-set of the first set of operators that the problem was correctly
diagnosed. But by then, major damage had been done.
The
operators had not been trained to understand the ambiguous nature of the PORV
indicator and look for alternative confirmation that the main relief valve was
closed. There was a temperature indicator downstream of the PORV in the tail
pipe between the PORV and the pressurizer that could have told them the valve
was stuck open, by showing that the temperature in the tail pipe remained high
after the PORV should have, and was assumed to have, shut, but this temperature
indicator was not part of the "safety grade" suite of indicators
designed to be used after an incident, and the operators had not been trained
to use it. Its location on the back of the desk also meant that it was effectively
out of sight of the operators.
Three Mile Island Nuclear Accident: Consequences of stuck
valve
As
the pressure in the primary system continued to decrease, reactor coolant
continued to flow, but it was boiling inside the core. First, small bubbles of
steam formed and immediately collapsed, known as nucleate boiling. As the
system pressure decreased further, steam pockets began to form in the reactor
coolant. This departure from nucleate boiling caused steam voids in coolant
channels, blocking the flow of liquid coolant and greatly increasing the fuel
plate temperature. The steam voids also took up more volume than liquid water,
causing the pressurizer water level to rise even though coolant was being lost
through the open PORV. Because of the lack of a dedicated instrument to measure
the level of water in the core, operators judged the level of water in the core
solely by the level in the pressurizer. Since it was high, they assumed that
the core was properly covered with coolant, unaware that because of steam
forming in the reactor vessel, the indicator provided false readings. This was
a key contributor to the initial failure to recognize the accident as a
loss-of-coolant accident, and led operators to turn off the emergency core
cooling pumps, which had automatically started after the initial pressure
decrease, due to fears the system was being overfilled.
With
the PORV still open, the quench tank that collected the discharge from the PORV
overfilled, causing the containment building sump to fill and sound an alarm at
4:11 a.m. This alarm, along with higher than normal temperatures on the PORV
discharge line and unusually high containment building temperatures and
pressures, were clear indications that there was an ongoing loss-of-coolant
accident, but these indications were initially ignored by operators. At 4:15,
the quench tank relief diaphragm ruptured, and radioactive coolant began to
leak out into the general containment building. This radioactive coolant was
pumped from the containment building sump to an auxiliary building, outside the
main containment, until the sump pumps were stopped at 4:39 a.m.
After
almost 80 minutes of slow temperature rise, the primary loop pumps began to
cavitate as steam, rather than water, began to pass through them. The pumps
were shut down, and it was believed that natural circulation would continue the
water movement. Steam in the system prevented flow through the core, and as the
water stopped circulating it was converted to steam in increasing amounts.
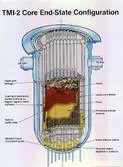
About 130 minutes after the first malfunction, the top of the reactor core was
exposed and the intense heat caused a reaction to occur between the steam
forming in the reactor core and the Zircaloy nuclear fuel rod cladding,
yielding zirconium dioxide, hydrogen, and additional heat. This fiery reaction
burned off the nuclear fuel rod cladding, the hot plume of reacting steam and
zirconium damaged the fuel pellets which released more radioactivity to the
reactor coolant and produced hydrogen gas that is believed to have caused a
small explosion in the containment building later that afternoon.
At
6 a.m., there was a shift change in the control room. A new arrival noticed
that the temperature in the PORV tail pipe and the holding tanks was excessive
and used a backup valve — called a block valve — to shut off the coolant
venting via the PORV, but around 32,000 US gal (120,000 L) of coolant had
already leaked from the primary loop. It was not until 165 minutes after the
start of the problem that radiation alarms activated as contaminated water
reached detectors; by that time, the radiation levels in the primary coolant
water were around 300 times expected levels, and the plant was seriously
contaminated.
Three Mile Island Nuclear Accident: Emergency declared
At
6:56 a.m., a plant supervisor declared a site emergency, and less than half an
hour later station manager Gary Miller announced a general emergency, defined
as having the "potential for serious radiological consequences" to
the general public. Metropolitan Edison notified the Pennsylvania Emergency
Management Agency (PEMA), which in turn contacted state and local agencies,
governor Richard L. Thornburgh and lieutenant governor William Scranton III, to
whom Thornburgh assigned responsibility for collecting and reporting on
information about the accident. The uncertainty of operators at the plant was
reflected in fragmentary, ambiguous, or contradictory statements made by Met Ed
to government agencies and to the press, particularly about the possibility and
severity of off-site radiation releases. Scranton held a press conference in
which he was reassuring, yet confusing, about this possibility, stating that
though there had been a "small release of radiation,... no increase in
normal radiation levels" had been detected. These were contradicted by
another official, and by statements from Met Ed, who both claimed that no
radiation had been released. In fact, readings from instruments at the plant
and off-site detectors had detected radiation releases, albeit at levels that
were unlikely to threaten public health as long as they were temporary, and
providing that containment of the then highly contaminated reactor was
maintained.
Angry
that Met Ed had not informed them before conducting a steam venting from the plant
and convinced that the company was downplaying the severity of the accident,
state officials turned to the NRC. After receiving word of the accident from
Met Ed, the NRC had activated its emergency response headquarters in Bethesda,
Maryland and sent staff members to Three Mile Island. NRC chairman Joseph
Hendrie and commissioner Victor Gilinsky initially viewed the accident, in the
words of NRC historian Samuel Walker, as a "cause for concern but not
alarm". Gilinsky briefed reporters and members of Congress on the
situation and informed White House staff, and at 10 a.m. met with two other
commissioners. However, the NRC faced the same problems in obtaining accurate
information as the state, and was further hampered by being organizationally
ill-prepared to deal with emergencies, as it lacked a clear command structure
and the authority to tell the utility what to do, or to order an evacuation of
the local area.
In
a 2009 article, Gilinsky wrote that it took five weeks to learn that "the
reactor operators had measured fuel temperatures near the melting point".
He further wrote: "We didn't learn for years—until the reactor vessel was
physically opened—that by the time the plant operator called the NRC at about 8
a.m., roughly one-half of the uranium fuel had already melted."
It
was still not clear to the control room staff that the primary loop water
levels were low and that over half the core was exposed. A group of workers
took manual readings from the thermocouples and obtained a sample of primary
loop water. Seven hours into the emergency, new water was pumped into the
primary loop and the backup relief valve was opened to reduce pressure so that
the loop could be filled with water. After 16 hours, the primary loop pumps
were turned on once again, and the core temperature began to fall. A large part
of the core had melted, and the system was still dangerously radioactive.
On
the third day following the accident, a hydrogen bubble was discovered in the
dome of the pressure vessel, and became the focus of concern. A hydrogen
explosion might not only breach the pressure vessel, but, depending on its
magnitude, might compromise the integrity of the containment vessel leading to
large scale release of radiation. However, it was determined that there was no
oxygen present in the pressure vessel, a prerequisite for hydrogen to burn or
explode. Immediate steps were taken to reduce the hydrogen bubble, and by the
following day it was significantly smaller. Over the next week, steam and
hydrogen were removed from the reactor using a catalytic recombiner and,
controversially, by venting straight to the atmosphere.