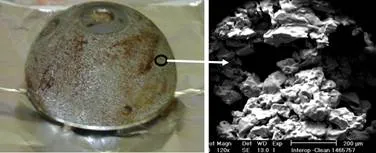
 Figure: An explanted Acetabulum cup (left). Right is a scanning electron microscope image of an of the implant that shows the surface roughness.
Figure: An explanted Acetabulum cup (left). Right is a scanning electron microscope image of an of the implant that shows the surface roughness.In 2000, Sulzer Orthopedics noticed higher than normal revision surgeries on their InterOpAcetabular Shell. The shell was held to the pelvis with screws, yet these sockets started to loosen. Patients experienced persistent and sharp groin pain due to this loosening and were unable to bear their weight on the leg that had the implant. Approximately 25,000 shells were affected. 17,500 of these were already implanted in patients. Following weeks of investigation of patients record, surgical techniques, and the product itself, the company ordered a recall. Sulzer eventually agreed to $1 billion settlement with affected patients.
Figure: An explanted Acetabulum cup (left). Right is a scanning electron microscope image of an of the implant that shows the surface roughness.
If you recall from my previous blog, during total hip replacement, an implant called acetabulum cup is inserted into the socket of the pelvic bone. The shell or socket mentioned in the Sulzer recall is this acetabulum cup. These acetabulum cups were cementless fixations. Their external surface undergoes a high-temperature treatment that increases the surface roughness. The increased surface roughness improves its integration with the surrounding tissue. Cemented fixations typically use polymethyl methacrylate polymer that interfaces between the implant which has a smoother surface, and the surrounding tissue.
The internal investigators at Sulzer isolated the high failure rate to specific manufacturing lots. The recalled products were manufactured between June 1997 through October 1999. Sulzer put together an independent research team comprising of pathologists, manufacturing experts, and analytical chemists. The team studied the surface properties of the implant as well as performed histopathological analysis of implant-tissue interface. The investigators suspected and eventually confirmed slight residue of a lubricant oil on the exterior porous surface of the shell which we believe can impede the bone from bonding to the shell.
The inflammatory response at the host tissue interface suggested absolute levels of the oil itself was the only reason for the host response. Tests showed that the failures were more prominent in implants had not undergone nitric acid passivation. Implants are treated with a mild oxidant such as nitric acid or citric acid solution as a final step. This treatment creates an oxide layer as a protective film that prevents corrosion or leaching of the metal ions that constitute the implants.
Studies also indicated that a substance in the oil, rather than the oil itself, was responsible for the inflammation. They noted that endotoxins elicit similar tissue response as that observed in the Inter-Op tissue. Endotoxins are toxic substance bound to the bacterial cell wall and released when the bacterium ruptures or disintegrates. After considering all the available information, the investigators concluded that the most likely reason for the host responses that lead to the loosening were adherent endotoxins that were delivered via the oil. In the absence of nitric acid treatment, these endotoxins are more prevalent leading to a greater inflammatory response. Nitric acid treatment under the conditions performed during the passivation reduces the levels of endotoxins but did not completely inactivate them.
Sulzer also made knee implants which also showed similar contamination with oil. However, the company did not recall those implants. They just replaced 229 out of the 1600 affected knee implants.
The case also raises interesting questions regarding organizational duties related to product liability.