Rh Blood Types
Rh blood types were discovered in 1940 by Karl
Landsteiner and Alexander Wiener. This was 40 years after Landsteiner had
discovered the ABO blood groups. Over the last half century, we have
learned far more about the processes responsible for Rh types. This blood
group may be the most complex genetically of all blood type systems since it
involves 45 different antigens on the surface of red cells that are controlled
by 2 closely linked genes on chromosome 1.
The Rh system was named after rhesus monkeys, since they were initially used in the research to make the antiserum for typing blood samples. If the antiserum agglutinates your red cells, you are Rh+ . If it doesn't, you are Rh- . Despite its actual genetic complexity, the inheritance of this trait usually can be predicted by a simple conceptual model in which there are two alleles, D and d. Individuals who are homozygous dominant (DD) or heterozygous (Dd) are Rh+. Those who are homozygous recessive (dd) are Rh- (i.e., they do not have the key Rh antigens).
Clinically, the Rh factor, like ABO factors, can lead to serious medical complications. The greatest problem with the Rh group is not so much incompatibilities following transfusions (though they can occur) as those between a mother and her developing fetus. Mother-fetus incompatibility occurs when the mother is Rh- (dd) and her fetus is Rh+ (DD or Dd). Maternal antibodies can cross the placenta and destroy fetal red blood cells. The risk increases with each pregnancy. Europeans are the most likely to have this problem--13% of their newborn babies are at risk. Actually only about ½ of these babies (6% of all European births) have complications. With preventive treatment, this number can be cut down even further. Less than 1% of those treated have trouble. However, Rh blood type incompatibility is still the leading cause of potentially fatal blood related problems of the newborn. In the United States, 1 out of 1000 babies are born with this condition.
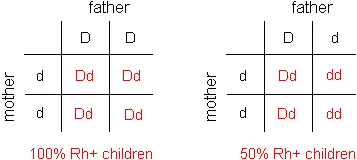
Rh type mother-fetus incompatibility occurs only when an Rh+ man fathers a child with an Rh- mother. Since an Rh+ father can have either a DD or Dd genotype, there are 2 mating combinations possible with differing risks as shown below. Regardless of the father's genotype, if he is Rh+ and the mother is Rh-, doctors assume that there will be an incompatibility problem and act accordingly.
|
|
|
|
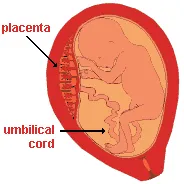
Human fetus in a mother's
uterus |
Keep in mind that only the Rh+ children (Dd) are likely to have medical complications. When both the mother and her fetus are Rh- (dd), the birth will be normal.
The first time an Rh- woman becomes pregnant, there usually are not incompatibility difficulties for her Rh+ fetus. However, the second and subsequent births are likely to have life-threatening problems for Rh+ fetuses. The risk increases with each birth. In order to understand why first born are normally safe and later children are not, it is necessary to understand some of the placenta's functions. It is an organ that connects the fetus to the wall of the uterus via an umbilical cord. Nutrients and the mother's antibodies regularly transfer across the placental boundary into the fetus, but her red blood cells usually do not (except in the case of an accidental rupture). Normally, anti-Rh+ antibodies do not exist in the first-time mother unless she has previously come in contact with Rh+ blood. Therefore, her antibodies are not likely to agglutinate the red blood cells of her Rh+ fetus. Placental ruptures do occur normally at birth so that some fetal blood gets into the mother's system, stimulating the development of antibodies to Rh+ blood antigens. As little as one drop of fetal blood stimulates the production of large amounts of antibodies. When the next pregnancy occurs, a transfer of antibodies from the mother's system once again takes place across the placental boundary into the fetus. The anti-Rh+ antibodies that she now produces react with the fetal blood, causing many of its red cells to burst or agglutinate. As a result, the newborn baby may have a life-threatening anemia because of a lack of oxygen in the blood. The baby also usually is jaundiced, fevered, quite swollen, and has an enlarged liver and spleen. This condition is called erythroblastosis fetalis . The standard treatment in severe cases is immediate massive transfusions of Rh- blood into the baby with the simultaneous draining of the existing blood to flush out Rh+ antibodies from the mother. This is usually done immediately following birth, but it can be done to a fetus prior to birth. Because the baby's own Rh+ red blood cells have been replaced with Rh- ones, the mother's anti-Rh+ antibodies don't agglutinate any additional red cells. Later, the Rh- blood will be replaced naturally as the baby gradually produces its own Rh+ blood. Any residual anti-Rh+ antibodies from the mother will leave gradually as well because the baby does not produce them.
Erythroblastosis fetalis can be prevented for women at high risk (i.e., Rh- women with Rh+ mates or mates whose blood type is unknown) by administering a serum (Rho-GAM ) containing anti-Rh+ antibodies into the mother around the 28th week of pregnancy and again within 72 hours after the delivery of an Rh+ baby. This must be done for the first and all subsequent pregnancies. The injected antibodies quickly agglutinate any fetal red cells as they enter the mother's blood, thereby preventing her from forming her own antibodies. The serum provides only a passive form of immunization and will shortly leave her blood stream. Therefore, she does not produce any long-lasting antibodies. This treatment can be 99% effective in preventing erythroblastosis fetalis. Rho-GAM is also routinely given to Rh- women after a miscarriage, an ectopic pregnancy, or an induced abortion. Without the use of Rho-GAM, an Rh- woman is likely to produce larger amounts of Rh+ antibodies every time she becomes pregnant with an Rh+ baby because she is liable to come in contact with more Rh+ blood. Therefore, the risk of life-threatening erythroblastosis fetalis increases with each subsequent pregnancy.
Anti-Rh+ antibodies may be produced in an individual with Rh- blood as a result of receiving a mismatched blood transfusion. When this occurs, there is likely to be production of the antibodies throughout life. Once again, Rho-GAM can prevent this from happening.
Mother-fetus incompatibility problems can result with the ABO system also. However, they are very rare--less than .1% of births are affected and usually the symptoms are not as severe. It most commonly occurs when the mother is type O and her fetus is A, B, or AB. The symptoms in newborn babies are usually jaundice, mild anemia, and elevated bilirubin levels. These problems in a baby are usually treated successfully without blood transfusions.